Abstract
Heart age summarizes multi-factorial cardiovascular risk into a single intuitive metric to motivate risk communication and prevention. Here, we present the design and validation of the Veevo Health Heart Age Calculator. Our calculator combines cardiovascular risk equations with a healthy age- and sex-matched comparator derived in part fromNational Health and Nutrition Examination Survey data (2015-2023). We apply our models to quantify population discordance between chronological age and heart age, finding that 1 in 5 adults (19.8%) have a heart age that exceeds chronological age by more than 10 years.
Introduction
Atherosclerotic cardiovascular disease (ASCVD) risk scores are essential for clinical decisionmaking. However, risks such as "7.5% within the next 10 years" can feel abstract and difficult to communicate [1]. Heart age instead asks: at what chronological age would an average healthy peer have the same predicted risk as this individual? This age-based framing acts as a mathematically consistent transformation of widely accepted risk equations [2], potentially improving patient communication and prevention adherence [3].
The Veevo Health Heart Age Calculator addresses this communication challenge while adhering to modern risk equations in an individualized manner. At a high level, we:
- Estimate an individual's 10-year ASCVD risk using validated, sex-specific equations.
- Derive healthy age- and sex-specific comparator risk profiles from population data.
- Solve for the comparator age where comparator risk equals the individual's risk.
Methods
Dataset
We downloaded data from the U.S. National Health and Nutrition Examination Survey (NHANES) 2015-2023 [4]. NHANES data was used to estimate healthy comparator parameters and describe national patterns of heart-age discordance. We combined cycles under the complex survey design and used Mobile Examination Center (MEC) weights, meaning survey-weighted estimates, so that all descriptive estimates and regression models reflect the US civilian, non-institutionalized population.
For readers who want the consumer-facing version of this work, the companion blog article explains the same findings in a lighter format, while the live calculator lets you estimate your own heart age.
Age- and sex-specific blood pressure
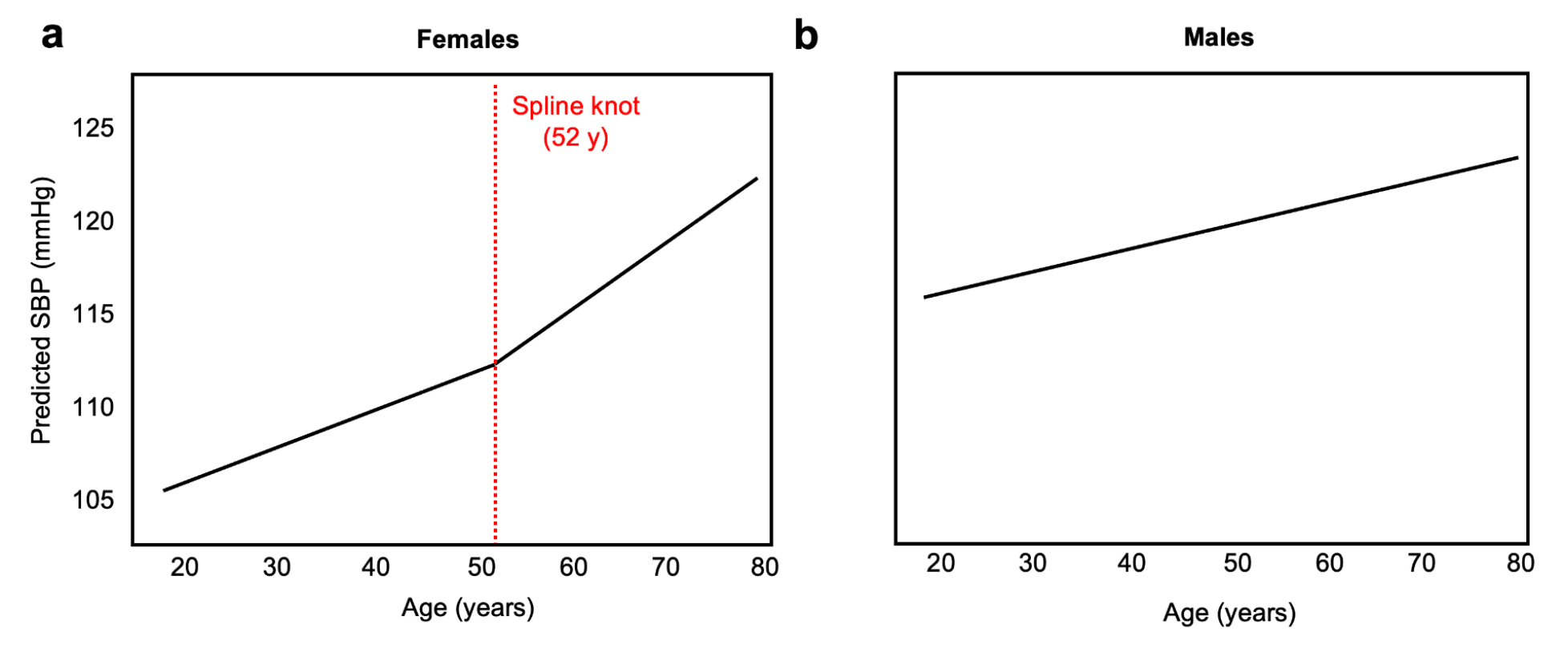
To derive systolic blood pressure (SBP) of low-risk individuals as a function of age and sex, we filtered the NHANES dataset to individuals with no history of tobacco use or diabetes, BMI < 30 kg/m2, SBP <140 mmHg, and no use of antihypertensive medications. We then fit sex-specific, survey-weighted models of SBP as a function of age (Figure 1). For females, we used a linear spline with a 52-year knot to reflect menopause physiology [2,5] (Fig. 1a). For males, we used linear regression (Fig. 1b).
Age- and sex-specific healthy comparator risk
Building on prior work from [2], our healthy comparator is defined as a subject who does not have diabetes, does not smoke or have smoking history, is not receiving lipid- or blood pressure-lowering therapy, and has intact renal function (eGFR = 90 mL/min/1.73m2). This health comparator also has lipid levels consistent with contemporary prevention goals [6], including high HDL-C (50 mg/dL for females, 45 mg/dL for males) and low non-HDL-C (115 mg/dL [7]). The SBP of the comparator is derived from an age- and sex-matched low-risk population using survey-weighted regression.
Risk model and heart age mapping
For each individual, we calculate individual risk using the basePREVENT 10-year risk equations [8]. We then solve for the age at which individual risk equals sex-matched healthy comparator risk.
Implementation guardrails
- The age input is restricted to ages 25-79 and the heart age solution is restricted to NHANES age bounds 18-79 years.
- Inputs are validated for physiological plausibility, with imputation of missing non-critical variables adhering to conservative, health-preserving values.
- Outputs display heart age and discordance with context-sensitive messaging to promote guideline-concordant prevention rather than risk minimization alone.
Population heart age discordance
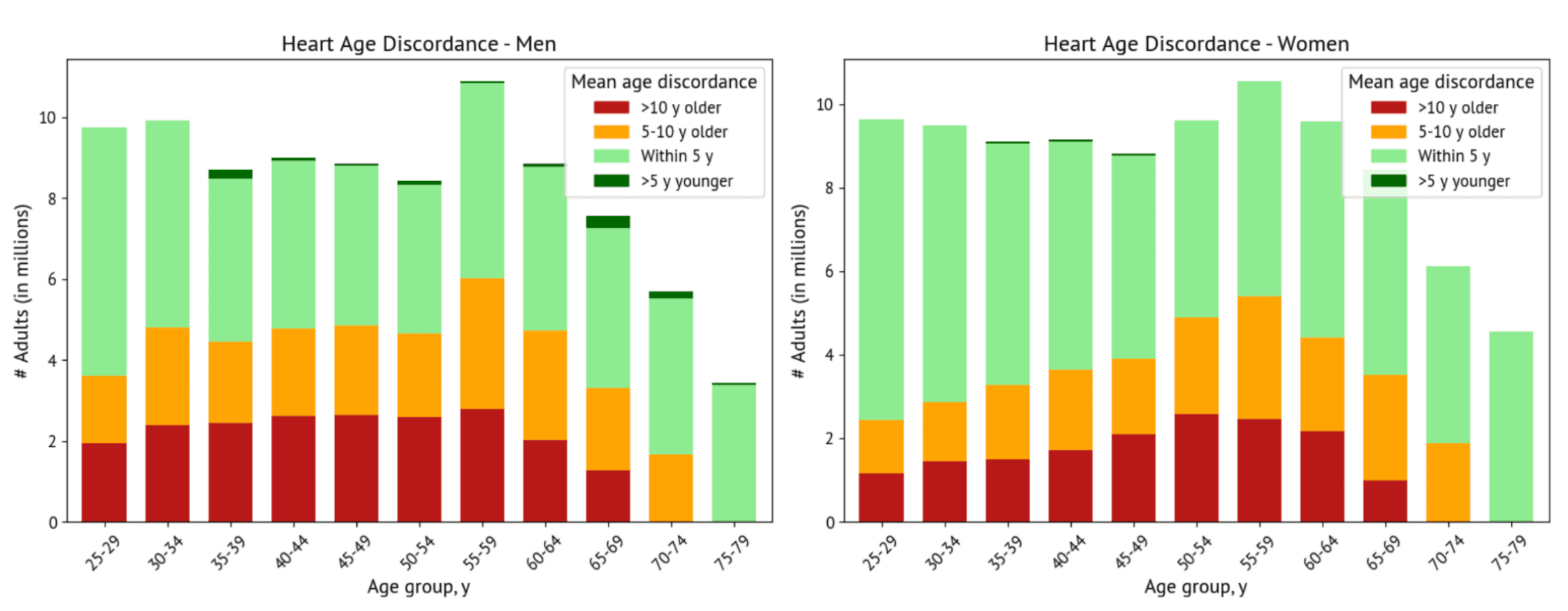
We calculated the heart age for all adults in the NHANES survey from age 25-79 years and quantified the difference between chronological age and heart age, with survey-weighted results consistent with the US population structure displayed (Figure 2, Table 1). Females have lower heart age discordance than men at younger ages but comparable discordance at older ages, consistent with increased lipids following menopause [9]. Heart age discordance declines after age 65, consistent with higher baseline cardiovascular risk even in healthy older adults [10].
Strikingly, more than 1 in 5 adults have a heart age more than 10 years older than their chronological age (Figure 2, Table 1). This may actually be an underestimate of true discordance and risk, as the current implementation constrains the model to return a maximum heart age of 79 and we do not include additional CVD risk factors, such as high Lipoprotein(a), bodily inflammation, and genetics.
Conclusion
The Veevo Health Heart Age Calculator translates complex risk into a validated intuitive number to encourage preventive action. This type of heart age calculator is especially useful for motivating prevention in younger individuals (less than 50 years), whose risk is underestimated in age-driven absolute risk calculators.
While our current calculator provides an important starting point, future work should seek to incorporate longitudinal medical data rather than point measurements and other variables that play an integral role in cardiovascular risk but are not captured in the PREVENT equations, including high-sensitivity C-reactive protein, apolipoprotein B, Lp(a), and imaging.
Personalized calculation and communication of cardiovascular risk is a key first step in population-level prevention, moving us toward a future free of heart disease.
Related resources: try the Veevo Heart Age Calculator, read the companion blog article, or learn more about our advanced heart CT program.
References
Waldron C-A, van der Weijden T, Ludt S, Gallacher J, Elwyn G. What are effective strategies to communicate cardiovascular risk information to patients? A systematic review. Patient Educ Couns. 2011;82: 169-181.
Blaha MJ, Naazie IN, Cainzos-Achirica M, Dardari ZA, DeFilippis AP, McClelland RL, et al. Derivation of a coronary age calculator using traditional risk factors and coronary artery calcium: The Multi-Ethnic Study of Atherosclerosis. J Am Heart Assoc. 2021;10: e019351.
Bonner C, Jansen J, Newell BR, Irwig L, Glasziou P, Doust J, et al. I don't believe it, but I'd better do something about it: patient experiences of online heart age risk calculators. J Med Internet Res. 2014;16: e120.
Paulose-Ram R, Graber JE, Woodwell D, Ahluwalia N. The National Health and Nutrition Examination Survey (NHANES), 2021-2022: Adapting data collection in a COVID-19 environment. Am J Public Health. 2021;111: 2149-2156.
Appiah D, Nwabuo CC, Ebong IA, Wellons MF, Winters SJ. Trends in age at natural menopause and reproductive life span among US women, 1959-2018. JAMA. 2021;325: 1328-1330.
Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, Garber AJ, et al. American Association of Clinical Endocrinologists and American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. 2017;23: 1-87.
Krishnan V, Huang X, Perak AM, Coresh J, Ndumele CE, Greenland P, et al. PREVENT risk age equations and population distribution in US adults. JAMA Cardiol. 2025;10: 962-964.
Khan SS, Matsushita K, Sang Y, Ballew SH, Grams ME, Surapaneni A, et al. Development and validation of the American Heart Association's PREVENT equations. Circulation. 2024;149: 430-449.
de Kat AC, Dam V, Onland-Moret NC, Eijkemans MJC, Broekmans FJM, van der Schouw YT. Unraveling the associations of age and menopause with cardiovascular risk factors in a large population-based study. BMC Med. 2017;15: 2.
Marma AK, Lloyd-Jones DM. Systematic examination of the updated Framingham heart study general cardiovascular risk profile. Circulation. 2009;120: 384-390.